Glaucoma is a collection of diseases that all have a final common effect. That effect is damage to the optic nerve. The optic nerve is a large nerve that exits from and attaches to the back of the eyeball. It is like a cable that takes the information from the eyeball to the brain. When damage occurs from glaucoma to the optic nerve, vision is lost. Typically, people lose vision above, below and slightly nasal to the center of vision.
Request an Appointment With Us or Give Us A Call Today

The images above represent formal visual field testing performed at the doctors office. The 2 left figures represent left eyes with inferior defects and the two figures on the right represent right eyes with superior defects. Put into real life situation the photograph of the couple below schematizes what can happen when glaucoma damage becomes advanced. The picture on the left is normal, but notice that the picture on the right has a “tunnel vision” appearance. This occurs when the defects detailed in the upper figures are present in together in one eye.

In advanced cases of glaucoma vision loss can extend into the central area and people become functionally, and legally blind. People often note other impacts to their vision as glaucoma progresses. Contrast sensitivity, or the ability to discriminate similar shades of colors is hampered. This can manifest in difficulty identifying each step on a stairwell. In addition, light/dark adaptation is slowed. This results in an abnormally prolonged time to adjust to new lighting conditions, like walking into a dimly lighted house from a sunny day.
The single greatest risk factor for, and often the direct cause of glaucoma is abnormally high eye pressure (normal eye pressure is below 21mmHg). During a comprehensive eye examination your doctor should check your pressure (above 21mmHg becomes suspicious), examine the front and backside of your eyes. Your doctor will be looking particularly at your optic nerve for signs of damage. Damage to the optic nerve takes on a certain “look” or appearance. In order for vision to be normal the eye must pressurize itself. There is a very elegant mechanism responsible for this pressurization and can be abnormal in multiple ways resulting in obstruction of the fluid from leaving the eye. This has resulted in glaucoma being classified into 2 categories:
- Open Angle Glaucoma
- Closed Angle Glaucoma
- For more information on glaucoma diagnosis and prevention, visit the American Glaucoma Society, the American Academy of Ophthalmology, and the Glaucoma Research Foundation
Open Angle Glaucoma
Open angle glaucoma is the most common form of glaucoma. It is characterized by an anatomically “open” drainage angle.
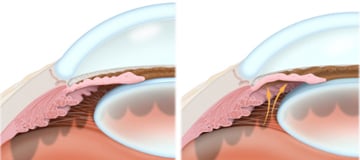
Notice in the left figure above that the space at the edge of the iris (where the iris connects to the eye wall) has a gap. This is called the trabecular meshwork and is the “drain” of the eye. The eye has an anatomically open angle. Contrast that with the eye in the right figure. The yellow arrows schematize the aqueous fluid as it pushes the iris toward the drain (trabecular meshwork) and “close” it. The eye in the right figure has an anatomically closed angle.
Primary Open Angle Glaucoma effects roughly 2% of the population, but up to 8% of people over 80. This disease does tend to run in families and having a first degree relative with glaucoma can increase your risk by up to 10 fold. Typically, there are no symptoms. For that reason it has been called the “Silent thief of vision”. The only way to know whether you have the disease or risk factors for the disease is to have your eyes examined.
Closed Angle Glaucoma
In contrast to open angle glaucoma, closed or narrow angle glaucoma is a less common. The primary form of angle closure glaucoma typically occurs in people with hyperopic eyes. Hyperopic eyes are anatomically “short” in comparison to an average eye. This situation results in a relative cramping of the structures of the eye.
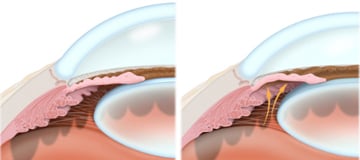
In the figures above, notice the drainage angle, which is the space just above the edge of the iris (brown part of the eye) marked with the arrow. The left figure shows a normal “open” angle, but the right figure shows anatomical closure. The problem occurs when 360 degrees of “plugging” occurs. The pressure quickly rises in the eye (above 21mmHg). This causes achy pain, redness, blurred vision, and swollen hazy cornea (the clear “watch glass” portion). Patients often experience “rainbow colored haloes” around lights. Also, the pupil will usually be mid-dilated and fixed. Many patients experience a headache that surrounds the eye during an attack. Also, people will often suffer from nausea and even vomiting.

Treatment of narrow angle glaucoma or prophylaxis against this event is demonstrated in the figures above. The left figure shows laser energy creating a hole, or ididotomy, to release the fluid trapped behind the iris. It is important to note that the laser iridotomy does not directly lower pressure in the eye. The iridotomy is designed to allow the fluid inside the eye a chance to get to the existing normal drains. If these drains have experienced damage that is too great they may not flow as much as is needed to achieve the desired pressure. In this situation your doctor may recommend medical or even more surgical therapy depending on the situation.
Glaucoma Therapy & Treatment
Glaucoma is treatable and numerous studies throughout the world have proven that lowering eye pressure delays progression of glaucoma. Currently, all therapies are aimed at lowering pressure, however numerous strategies aimed at neuro-protection have been considered without success. Lowering eye pressure can be achieved by either decreasing the amount of fluid being created inside the eye or by increasing the amount of fluid that gets out of the eye.
There are 3 categories of glaucoma treatment:
- Medicines
- Lasers
- Filtration Surgeries